
联系电话:025-84541951
地址:南京市秦淮区白下路273号

江苏省老年医学学会老年内分泌专业委员会、江苏省医学会糖尿病学分会、江苏省预防医学会糖尿病预防与控制专业委员会、南京糖尿病并发症研究会老年分会
通讯作者:唐伟,江苏省老年病医院内分泌科,南京,210024,Email: drtangwei@njmu.edu.cn,马向华,江苏省人民医院内分泌科,南京,210029,Email: 13952002505@139.com
关键词:2型糖尿病,老年,SGLT-2抑制剂,专家共识
老年人群糖尿病患病率高,合并多种基础疾病或代谢异常的比率高,心脑血管死亡和慢性肾脏病发生风险增加,常多重用药且对药物不良反应的耐受性差,因此,在选择降糖药物时需综合评估患者病情,加强用药指导及治疗后的监测。已有多项研究证实,SGLT-2i除具有良好的降糖作用外,还具有确切的心血管和肾脏保护作用。本共识汇总SGLT-2i的种类特点、降糖及降糖外作用、安全性与依从性,以提升临床医生对该类药物的全面了解,指导在老年糖尿病人群中的合理使用。
一、老年2型糖尿病流行病学及其特点
我国老年人群的糖尿病患病率随年龄增长,进入老年后罹患糖尿病的风险增高。2017年的流行病学调查显示,我国60岁以上老年糖尿病患病率为30.0%,女性高于男性,且95%以上为2型糖尿病(T2DM)[1]。老年糖尿病可分为老年前患病(约占30%)及老年后患病(约占70%)两类。不同年龄起病的老年糖尿病患者的临床特征存在差异。与老年前患病者相比,老年后患病者伴心血管病风险因素及肾功能损害均更多,而伴糖尿病视网膜病变较少[2,3]。
心脑血管疾病、肾衰竭、恶性肿瘤及肺部感染是老年糖尿病主要致亡病因[4]。高血压和血脂紊乱是老年人心脑血管死亡的最主要危险因素。中国3B 研究显示,约72%的糖尿病患者合并高血压和血脂紊乱[5],三者并存将使心脑血管死亡风险增加3倍[6]。动脉粥样硬化性心血管疾病(ASCVD)在老年患者中具有高发病率、高致残率和高病死率的特点[7],且ASCVD患病率随年龄增长而升高[8]。国内一项针对上海市高行社区的调查显示,老年人群ASCVD患病率为21.51%[9]。另外,60岁以上老年人群慢性肾脏病(CKD)的患病率高达33%[10],且老年人群中,CKD通常与多种合并症、心血管高风险以及虚弱、残疾和营养不良的患病率增加有关[11,12]。
二、SGLT-2i应用现状、获益和风险
新近国内外指南均推荐[13,14],当T2DM患者合并ASCVD或CV高危因素、HF或CKD时,不论其HbA1c是否达标,建议优先联合具有心、肾获益证据的钠-葡萄糖协同转运蛋白2(sodium-glucose cotransporter-2, SGLT2)抑制剂或胰高血糖素样肽-1(glucagon-like peptide-1, GLP-1)受体激动剂。
SGLT-2i通过选择性抑制SGLT2,减少葡萄糖重吸收,降低肾糖阈,增加尿糖排泄,以非胰岛素依赖的方式降低血糖水平。 近年来,一系列心血管病和肾脏病结局的大型临床研究证实,SGLT-2i显著降低T2DM合并心血管高危风险者的主要心血管不良事件及心力衰竭住院率[15,16];在并发糖尿病肾脏病(DKD)的患者中,SGLT-2i能减轻蛋白尿,显著降低肾脏事件复合终点发生[16,17]。
尽管目前尚缺乏针对老年糖尿病人群的独立RCT研究证据,但研究中老年亚组的荟萃分析显示,SGLT-2i能有效改善其血糖、血压及体重[18]。EMPA-REG OUTCOME及DECLARE-TIMI 58研究的老年亚组分析亦证实了此类药物对老年患者的心血管获益[19]。然而,SGLT-2i常见不良反应为泌尿生殖系统感染,还有引起血容量不足、酮症酸中毒、骨折、急性肾损伤的潜在风险[20]。由于老年患者通常病程长、基础疾病多、对药物不良反应的耐受性差,因此启用此类药物需综合评估病情,加强用药指导及治疗后的监测。
三、SGLT-2i的降糖及降糖外作用
1.降糖作用
SGLT-2i通过单药或联合用药,可使尿糖排泄增加至每日70g - 80g,使糖化血红蛋白降低0.3% - 1.2%[21]。荟萃分析显示,老年患者使用SGLT-2i可使糖化血红蛋白降低0.4%,与年轻组相比无明显差异,提示SGLT-2i的降糖效应不受年龄影响[18]。
1.1单药治疗
SGLT-2i单药治疗时,糖化血红蛋白降幅与其基线值及SGLT2i剂量密切相关[21]。以达格列净为例,分别使用达格列净2.5mg、5mg、10mg每天一次治疗24周,可使糖化血红蛋白降低0.58%、0.77%、0.89%,且糖化血红蛋白基线值越高,其降幅越明显[22]。卡格列净100mg,300mg每天一次单药治疗26周后,糖化血红蛋白分别降低0.77%和1.03%,空腹血糖分别降低2.0mmo/L和2.4mmo/L,餐后2小时血糖分别降低2.7mmo/L和3.6mmo/L,上述效应可持续至用药后52周[23]。
1.2联合用药
对于二甲双胍单药治疗控制不佳的患者,加用SGLT-2i治疗,可使糖化血红蛋白降低0.5%-0.9%[24]。荟萃分析比较了二甲双胍控制不佳后,分别联用达格列净、噻唑烷二酮、磺脲类、DPP4抑制剂,发现其降糖作用相当,并且相对于磺脲类,达格列净等其他三组低血糖风险相对降低[25]。恩格列净与二甲双胍联合治疗24周,安慰剂组糖化血红蛋白较基线水平降低0.13%,恩格列净10mg组糖化血红蛋白降低0.7%,25mg组糖化血红蛋白降低0.77%。对于糖化血红蛋白基线>10%的患者,25mg恩格列净组糖化血红蛋白较基线降低3.2%[26]。SGLT-2i与胰岛素或其他口服降糖药联用,可使糖化血红蛋白进一步降低0.4%-1.1%[27,28]。如达格列净联合吡格列酮治疗24周后,5mg和10mg组糖化血红蛋白水平分别降低0.82%和0.97%[27]。一项针对老年T2DM患者的真实世界研究显示,SGLT-2i联合GLP-1受体激动剂治6个月后,糖化血红蛋白水平较基线降低1.1%(P<0.001),且基线糖化血红蛋白>8.4%的患者有更大获益[28]。
2.其他代谢改善作用
2.1体重
SGLT-2i主要是通过热量损失及渗透性利尿导致体重减轻[29]。多项荟萃分析显示,与安慰剂相比,SGLT-2i能显著降低老年人体重,不同研究背景的减重效果存在差异,综合减重效果为1.72 kg[18]。55-80岁老年T2DM患者每天100mg或300mg卡格列净,随访104周可观察到体重平均减轻2.7kg或3.5kg[30];65岁及以上的T2DM患者,达格列净每天10mg 24周可减重2.6kg,减重作用持续52周[31]。SGLT-2i的减重效果在治疗初期几周最明显,而后逐渐趋缓,体重指数越大,体重减轻越多。与其他具有减重作用的降糖药物如GLP-1受体激动剂联用时,减重作用具有叠加性[32-35]。此外,SGLT-2i能改变身体成分,并增加胰岛素敏感性,有利于肌肉组织的合成代谢[36,37]。一项达格列净治疗超过 102周的研究发现,受试者治疗后内脏脂肪和皮下脂肪明显减少,且体重下降的2/3为脂肪、1/3为去脂体重[38]。
2.2血脂
SGLT-2i对血脂的影响结论不一。有研究表明,SGLT-2i 可降低甘油三酯(TG)及低密度脂蛋白胆固醇(LDL-C),升高高密度脂蛋白胆固醇(HDL-C), 但不增加LDL/HDL比值[33,39,40]。在EMPA-REG OUTCOME 研究中,恩格列净仅与LDL-C 和HDL-C 的轻度增加有关,但无临床意义[41]。因此SGLT-2i对血脂的影响还需进一步研究证实。
2.3血压
多项针对老年人群的研究表明,单独应用SGLT-2i能有效降低血压[30,42,43]。荟萃分析结果显示,与安慰剂比较,SGLT-2i可使T2DM合并高血压患者24 h动态收缩压降低4.36 mmHg,舒张压降低2.20 mmHg,卡格列净、达格列净、恩格列净和艾托格列净分别可使收缩压降低4.59 mmHg、3.74 mmHg、5.06 mmHg和3.64 mmHg,舒张压降低2.30 mmHg、1.22 mmHg、2.00 mmHg和2.69 mmHg[44]。目前,SGLT-2i 的降压原因包括渗透性利尿、肾单位重构、血管炎症及内皮功能改善、体重减轻等[45]。
2.4尿酸
SGLT-2i 降低尿酸的机制可能更多归因于通过葡萄糖转运蛋白9(GLUT9)转运促进尿酸排泄[46]。卡格列净、恩格列净、达格列净均可降低尿酸水平,平均可降低37.73μmol/L,其中恩格列净降低尿酸效果最显著,可降低约45.83 μmol/L[47]。SGLT-2i降低血尿酸作用主要受血尿酸、糖化血红蛋白及糖尿病病程影响,血尿酸及糖化血红蛋白水平越高、糖尿病病程越短,其降尿酸作用越强[48,49]。
3. 心肾获益
动脉粥样硬化性心血管疾病(ASCVD)是糖尿病患者的主要死因之一,高血压和血脂异常是ASCVD的明确危险因素,而糖尿病本身就是冠心病等危症。控制个体心血管危险因素可有效预防或延缓糖尿病患者ASCVD的发生发展。多项大型随机、双盲、安慰剂对照试验结果显示,对合并ASCVD或有心血管高危风险的T2DM患者,SGLT-2i具有心血管获益,并减缓慢性肾脏病的进展。分层分析表明,老年患者与年轻患者相比具有相似或更大益处。
3.1 不同SGLT-2i的心血管结局(CVOT)研究比较
目前已公布的SGLT-2i的CVOT研究[41,50-52]结果显示,仅恩格列净和卡格列净具有3P-MACE获益,卡格列净是唯一在心血管一级和二级预防人群均具有3P-MACE获益的SGLT-2i。EMPA-REG OUTCOME研究显示,恩格列净组≥65岁的老年人群亚组较<65岁的老年人群亚组降低3P-MACE风险的效果更好[41]。CANVAS研究中,卡格列净组≥65岁的老年人群亚组与<65岁的老年人群亚组降低3P-MACE风险获益一致[50]。
3.2 不同SGLT-2i在T2DM合并心衰患者的获益比较
约50%的T2DM患者可能出现心力衰竭[53],通常导致不良预后。糖尿病合并心衰或心衰高风险患者在确定治疗方案时,应谨慎考虑降糖药物与心力衰竭相关的风险和益处。目前常用的4个SGLT-2i在T2DM合并心衰患者存在不同程度的获益,以恩格列净、卡格列净、达格列净的心衰获益为佳,而降低心衰住院风险获益一致[41,50-52]。
3.3 不同SGLT-2i改善T2DM合并CKD患者肾脏复合终点的比较
卡格列净的CREDENCE研究[54]、恩格列净的EMPA-REG OUTCOME研究[41]、达格列净的DAPA-CKD研究[55]以及艾托格列净的VERTIS CV研究[52]均显示,与安慰剂相比,SGLT-2i可显著改善T2DM合并CKD患者肾脏复合终点。
综上,有关SGLT-2i的心血管结局研究、心衰结局研究及肾脏结局研究的老年亚组的分析结果均提示,SGLT-2i的应用和获益基本不受年龄和糖尿病病程的影响,尤其在合并心衰和CKD患者获益更多。
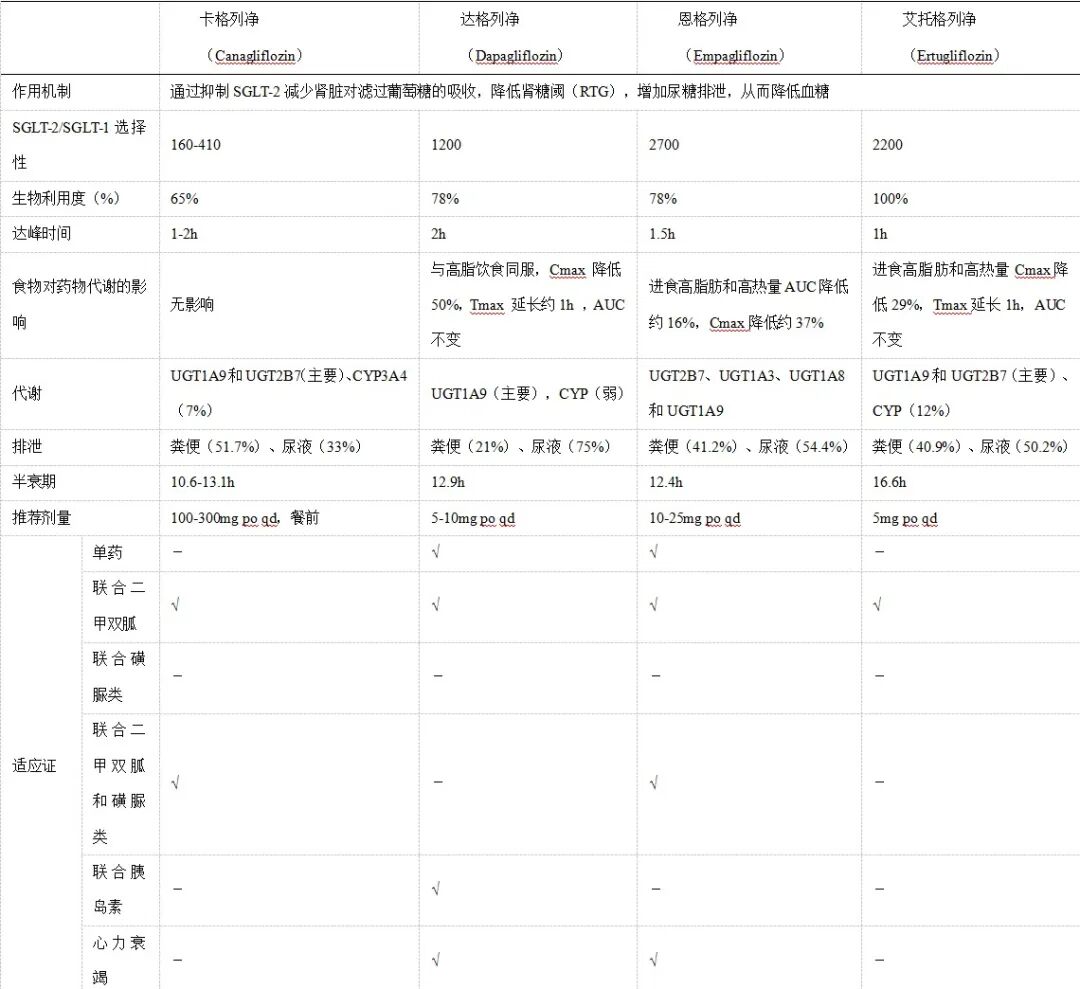
四、SGLT-2i种类、作用特点及适应证
表1 SGLT-2i种类、作用特点及适应证
五、SGLT-2i在老年T2DM使用注意事项
不推荐SGLT-2i用于T1DM、儿童青少年、孕妇和哺乳期妇女以及糖尿病酮症酸中毒、高糖高渗状态;其在老年T2DM患者中使用时应注意以下事项:
(1)低血糖:SGLT-2i单药治疗不增加低血糖发生风险。与二甲双胍、二肽基肽酶- 4抑制剂(DPP4i)、噻唑烷二酮等药物联合使用时,低血糖发生风险也没有明显增加;与胰岛素或磺脲类药物联合使用时低血糖发生风险增加。
(2)肾功能不全:老年人由于衰老等原因致肾小球滤过率的自然下降,老年糖尿病患者更易发生肾功能不全。临床医生在起始SGLT-2i治疗前应评估患者肾功能,处方后也需要定期监测该指标。恩格列净、达格列净和卡格列净不建议在eGFR持续低于45 mL/min/1.73m2的患者中使用;已接受上述SGLT-2i治疗的患者如果eGFR低于30 mL/min/1.73m2,则应停止继续使用。艾托格列净则不应在eGFR 持续低于 60 mL/min/1.73m2的患者中起始或继续使用。对于伴或不伴T2DM的心力衰竭患者,如30≤eGFR<45 ml/min/1.73 m2,可使用达格列净或恩格列净10mg/天;已接受上述SGLT-2i治疗的患者如果eGFR低于30 mL/min/1.73m2,则应停止使用。对于CKD患者,eGFR<25 ml/min/1.73 m2如已服用达格列净,则继续使用。所有SGLT-2i禁用于透析患者(见表2)。
表2 肾功能不全患者SGLT-2i剂量调整
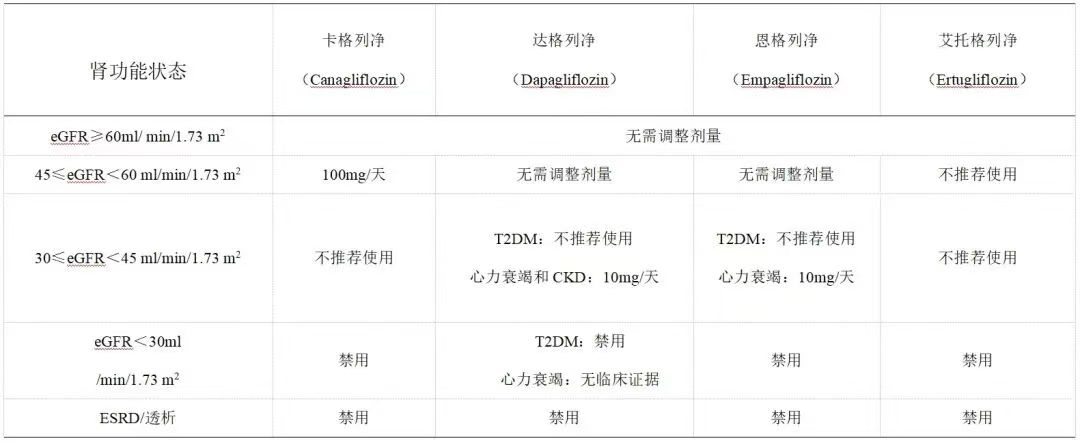
注:eGFR:估测的肾小球滤过率;T2DM:2型糖尿病;ESRD:终末期肾病。
急性肾损伤患者,SGLT-2i可引起血容量下降,可能是引起肾功能损害的原因。在使用之前,须考虑容易出现急性肾损伤的因素,包括低血容量、慢性肾功能不全、充血性心力衰竭以及相关用药(利尿剂、ARB、NSAID)。若经口摄入减少或存在液体丢失,应考虑暂停使用SGLT-2i。观察患者是否出现急性肾损伤的症状和体征,如果出现急性肾损伤,应立即停用,并开始治疗。
(3)血容量不足与低血压:与血容量不足相关的不良事件包括低血压、直立性低血压、脱水、头晕和晕厥等。由于SGLT-2i可引起渗透性利尿,特别是老年患者,由于体液调节的改变和液体摄入量的减少,更容易发生SGLT-2i相关的血容量减少事件,特别是同时接受袢利尿剂的患者[19]。血容量不足事件发生率可随着肾功能的恶化而增加,CKD 2期为1.0%,CKD 3期为3.7%,CKD 4期为5.4%[56]。在老年人中,必须特别注意直立性低血压,使用SGLT-2i后其发生率增加高达9%[57]。血容量相对不足导致体位性低血压、体位性眩晕、晕厥等情况发生,使意外跌倒风险增加从而发生骨折。
因此,在老年、肾功能受损(eGFR低于60 mL/min/1.73 m2)、血压较低、使用肾素-血管紧张素-醛固酮系统阻滞剂或正服用袢利尿剂的患者在开始SGLT-2i治疗前,应评估血容量状态和肾功能,在治疗期间应监测低血压的体征和症状以及肾功能[18]。
(4)泌尿、生殖系统感染:SGLT-2i促进大量葡萄糖从尿液中排出,增加泌尿生殖道局部的葡萄糖浓度,导致发生细菌和霉菌感染的机会增加,且在女性中发生率相对较高。在SGLT-2i使用过程中,如果发生感染并需要抗感染治疗时建议暂停使用,感染治愈后可继续使用。半年内反复发生泌尿生殖感染的患者不推荐使用。服用SGLT-2i的患者,应适量饮水,个人外阴清洁,减少感染的发生。
SGLT-2i抑制剂可导致Fournier's 坏疽(生殖器或会阴坏死性筋膜炎)的发生风险,泌尿生殖道感染或会阴脓肿可能先于坏死性筋膜炎,如果患者在生殖器或会阴部位出现剧烈疼痛,压痛,红斑或肿胀,伴有发热或不适,建议患者寻求紧急医疗护理。
(5)酮症及酮症酸中毒:SGLT-2i相关的DKA常常是正常血糖性DKA,大多发生于胰岛素缺乏的糖尿病患者,诱因多为手术、过度运动、心肌梗死、极低碳水化合物摄入等应激事件。在使用SGLT-2i期间,如果出现和糖尿病酮症相关症状,如腹痛、恶心、呕吐、乏力、呼吸困难等,需要检测血酮体和动脉血酸碱度以明确诊断。明确诊断为糖尿病酮症后,应停用SGLT-2i,并针对糖尿病酮症进行治疗。启用SGLT-2i时可采取以下措施防止DKA发生:避免胰岛素剂量不足或中断使用;在择期手术或侵入性手术前、严重急性疾病或感染期间暂停使用该类药物≥72小时;避免过度饮酒和生酮饮食[58,59]。
(6)老年肌少症:使用SGLT-2i可引起体成分变化,现有证据表明这类药物所致的体质量改变主要是脂肪量的降低[38]。然而,体质量减少是否增加肌少症风险值得引起重视。目前不同研究关于使用SGLT-2i是否导致糖尿病患者发生肌少症的结果并不一致[60,61],尚无法确定SGLT-2i与肌少症的相关性。有研究发现,长期使用SGLT-2i可能导致肌少症发病率升高[60]。另一项日本研究显示,T2DM患者使用达格列净治疗6个月可显著降低体质量和脂肪量,而治疗前后瘦组织含量、骨骼肌量及骨骼肌指数均无显著降低,提示达格列净在降低体质量同时对肌量无明显影响[61]。
(7)骨质疏松:SGLT-2i会增加肾小管对磷的重吸收,可能影响钙磷代谢,使血磷升高,刺激甲状旁腺素的分泌,从而增强骨吸收,对骨代谢产生不利影响。加拿大卫生部的安全性审查发现,使用卡格列净与骨骼相关的副作用存在联系,而使用达格列净仅在有肾脏问题的患者中发现骨折风险。但是,Meta分析结果不支持使用SGLT-2i增加T2DM 患者发生骨折风险[62,63]。尽管使用SGLT-2i与骨折风险之间的关系仍有待明确,SGLT-2i引起的减重使骨骼负荷减少及肌肉脂肪合成代谢减少造成的骨丢失可能是影响骨密度(BMD)的重要因素,而低 BMD 是骨折发生的重要危险因素[64]。因此,SGLT-2i在骨折高风险人群中仍应谨慎使用,如绝经后妇女或骨质疏松患者。
(8)药物相互作用:老年T2DM患者常为多病共存,服用多种治疗药物,需注意药物间的相互作用。SGLT-2i主要通过尿苷二磷酸葡醛酸转移酶(UGT)代谢,达格列净、卡格列净和艾托格列净极少量经细胞色素P450酶(CYP450酶)代谢,故与肝酶诱导剂/抑制剂几乎无相互作用(见表1)。
与口服降糖药和降压药联用
SGLT-2i在联合使用其他降糖药、降压药等药物时,药代动力学参数AUC和Cmax仅受到少量影响,AUC的变化均不影响SGLT-2i联合用药的临床疗效,无需调整SGLT-2i和联合用药的剂量[65-69]。值得注意的是,卡格列净300mg增加地高辛Cmax达36%,联用时应密切监测地高辛血药浓度。一项meta分析表明,使用卡格列净的患者与达格列净(10mg)和恩格列净(10mg)相比,与胰岛素和磺脲类药物联用发生低血糖的风险增加[70]。
与其他药物联用
利福平联合使用卡格列净时,能降低卡格列净的AUC达 51%,可能降低卡格列净的疗效[66]。如果卡格列净与UGT诱导剂(如利福平、苯妥英、苯巴比妥和利托那韦)联合使用,则对于耐受本品100mg每天一次剂量、eGFR>60 ml/min/1.73 m2且需要额外血糖控制的患者,可考虑增加剂量至300 mg每天一次;对于eGFR为45至<60 ml/min/1.73 m2,联合使用UGT诱导剂且需要额外血糖控制的患者,可考虑其他降糖治疗[71]。利福平增加恩格列净的AUC35%、降低达格列净AUC22%、降低艾托格列净 AUC39%和Cmax 15%,但是对临床疗效无显著的影响。
与食物的相互作用
多项研究[72-75]表明,与空腹状态相比,高脂肪餐对SGLT-2i的药动学没有临床意义的影响,可以空腹或者餐后服用SGLT-2i。由于卡格列净亦可抑制SGLT-1延缓肠道葡萄糖的吸收,从而降低餐后血糖波动,建议卡格列净最好在每天第一餐前服用。
五、小结与展望
老年T2DM患者常伴有肥胖、高血压及高尿酸血症等多重代谢异常,心血管疾病和慢性肾脏病变的患病比例也较高。SGLT-2抑制剂作为常用口服降糖药物,因其良好的降糖效果、降低血压、降低血尿酸、减轻体重和心肾保护作用而越来越受到关注。越来越多的证据显示,SGLT-2抑制剂能够显著改善血糖及多种代谢异常,降低心衰发生风险,减少蛋白尿并延缓eGFR降低速率。在应用过程中,应严格掌握好单药及联合用药适应证。良好的生活习惯可有效降低生殖道及泌尿系统的感染风险。在胰岛功能较差的患者使用时,需给予适量补充胰岛素治疗,警惕酮症的发生。
编写顾问(按姓氏笔画排序)
成兴波(苏州大学附属第一医院内分泌科)
刘超(江苏省中西医结合医院内分泌科)
杨涛(江苏省人民医院内分泌科)
执笔(按姓氏笔画排序)
俞匀(江苏省老年病医院内分泌科)
智俊娜(江苏省老年病医院药学部)
编写组成员(按姓氏笔画排序)
王爱萍(东部战区空军医院内分泌科)
王雪琴(南通市第一人民医院内分泌科)
方小正(江苏省淮安市第一人民医院老年医学科)
毕艳(南京大学医学院附属南京鼓楼医院内分泌科)
李玲(东南大学附属中大医院内分泌科)
陆婧(南京大学医学院附属鼓楼医院内分泌科)
胡吉(苏州大学附属第二医院内分泌科)
娄青林(江苏省老年病医院内分泌科)
祝群(南京医科大学第二附属医院内分泌科)
姚伟峰(无锡市第二人民医院内分泌科)
袁国跃(江南大学附属医院内分泌科)
顾刘宝(江苏省老年病医院内分泌科)
鲁一兵(南京医科大学第二附属医院内分泌科)
参考文献
Li Y, Teng D, Shi X, et al. Prevalence of diabetes using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study[J]. BMJ, 2020, 369:m997.
LeRoith D, Biessels GJ, Braithwaite SS, et al. Treatment of diabetes in older adults: an Endocrine Society* clinical practice guideline[J]. J Clin Endocrinol Metab, 2019,104(5):15201574.
Selvin E, Coresh J, Brancati FL. The burden and treatment of diabetes in elderly individuals in the u. s[J]. Diabetes Care, 2006, 29(11):24152419.
《中国老年2 型糖尿病防治临床指南》编写组.中国老年2型糖尿病防治临床指南(2022年版)[J].中国糖尿病杂志, 2022, 30(1):2-51.
Ji L, Hu D, Pan C, et al. Primacy of the 3B approach to control risk factors for cardiovascular disease in type 2 diabetes patients[J]. Am J Med, 2013, 126(10): 925. e11-22.
苏俊, 田慧, 李春霖, 等. 老年糖尿病住院患者死亡原因分析[J].第一军医大学学报, 2004,24(1):110-112.
Zheng L,Lan Q,Zhang Y,et al. The screening value of baPWV and hs-crp to ASCVD in middle and elderly community population in Shanghai[J]. Int J Cardiol, 2015,186:289-290.
Schiros CG, Denney TS,Gupta H. Interaction analysis of the new pooled cohort equations for 10-year atherosclerotic cardiovascular disease risk estimation: a simulation analysis[J]. BMJ Open,2015,5(4):e006468.
郑亮, 吴宏, 钱定广,等.上海市高行老年社区人群动脉硬化性心血管疾病患病率的现况调查与危险因素分析[J].中国循证心血管医学杂志, 2016,8(6): 680-682, 690.
D'Alessandro C, Piccoli GB, Barsotti M,et al. Prevalence and Correlates of Sarcopenia among Elderly CKD Outpatients on Tertiary Care[J]. Nutrients, 2018, 10(12): 1951.
Kooman JP, van der Sande FM, Leunissen KM.Kidney disease and aging: A reciprocal relation[J].Exp Gerontol, 2017,87(Pt B):156-159.
Lee SJ, Son H, Shin SK.Influence of frailty on health-related quality of life in pre-dialysis patients with chronic kidney disease in Korea: A cross-sectional study[J].Health Qual Life Outcomes, 2015,13:70.
中华医学会糖尿病学分会.中国2型糖尿病防治指南(2020年版)[J].中华糖尿病杂志,2021,13(4):315-409.
American Diabetes Association. Standards of medical care in diabetes-2022[J]. Diabetes Care, 2022, 45(Suppl 1): S135-S137.
Usman MS, Siddiqi TJ, Memon MM, et al. Sodium-glucose co-transporter 2 inhibitors and cardiovascular outcomes: A systematic review and meta-analysis[J].Eur J Prev Cardiol, 2018,25(5):495-502.
Zelniker TA, Braunwald E. Clinical Benefit of Cardiorenal Effects of Sodium-Glucose Cotransporter 2 Inhibitors: JACC State-of-the-Art Review[J]. J Am Coll Cardiol, 2020,75(4):435-447.
Muskiet MHA, Wheeler DC, Heerspink HJL. New pharmacological strategies for protecting kidney function in type 2 diabetes[J]. Lancet Diabetes Endocrinol, 2019,7(5):397-412.
Cintra R, Moura FA, Carvalho LSF, et al. Inhibition of the sodium-glucose co-transporter 2 in the elderly: clinical and mechanistic insights into safety and efficacy[J]. Rev Assoc Med Bras (1992), 2019,65(1):70-86.
Custódio JS Jr, Roriz-Filho J, Cavalcanti CAJ, et al. Use of SGLT-2 Inhibitors in Older Adults: Scientific Evidence and Practical Aspects[J]. Drugs Aging, 2020,37(6):399-409.
Lin DS, Lee JK, Chen WJ. Clinical Adverse Events Associated with Sodium-Glucose Cotransporter 2 Inhibitors: A Meta-Analysis Involving 10 Randomized Clinical Trials and 71 553 Individuals[J]. J Clin Endocrinol Metab, 2021,106(7):2133-2145.
Miller EM. Elements for Success in Managing Type 2 Diabetes With SGLT-2 Inhibitors: Individualizing Treatment With SGLT-2 Inhibitor Therapy in Type 2 Diabetes Mellitus[J]. J Fam Pract, 2017, 66(2 Suppl):S13-S16.
Ferrannini E, Ramos SJ, Salsali A, et al. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: a randomized, double-blind, placebo-controlled, phase 3 trial[J]. Diabetes Care, 2010, 33(10):2217 -2224.
Stenlöf K, Cefalu WT, Kim KA, et al. Long-term efficacy and safety of canagliflozin monotherapy in patients with type 2 diabetes inadequately controlled with diet and exercise: findings from the 52-week CANTATA-M study[J]. Curr Med Res Opin, 2014, 30(2):163-175.
Tsushima Y, Lansang MC, Makin V. The role of SGLT-2 inhibitors in managing type 2 diabetes[J]. Cleve Clin J Med, 2021, 88(1):47-58.
Goring S, Hawkins N, Wygant G, et al. Dapagliflozin compared with other oral anti-diabetes treatments when added to metformin monotherapy: a systematic review and network meta-analysis[J]. Diabetes Obes Metab, 2014, 16(5):433-442.
Häring HU, Merker L, Seewaldt-Becker E, et al. Empagliflozin as add-on to metformin in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial[J]. Diabetes Care, 2014, 37(6):1650-1659.
Rosenstock J, Vico M, Wei L, et al. Effects of dapagliflozin, an SGLT2 inhibitor, on HbA(1c), body weight, and hypoglycemia risk in patients with type 2 diabetes inadequately controlled on pioglitazone monotherapy[J]. Diabetes Care, 2012,35(7):1473-1478.
Carretero Gómez J, Arévalo Lorido JC, Gómez Huelgas R, et al. Combination Therapy With Glucagon-Like Peptide-1 Receptor Agonists and Sodium-Glucose Cotransporter 2 Inhibitors in Older Patients With Type 2 Diabetes: A Real-World Evidence Study[J]. Can J Diabetes, 2019, 43(3):186-192.
张洁,郭立新.钠-葡萄糖共转运蛋白2抑制剂改善体重的特点、影响因素及其机制[J].中华糖尿病杂志,2019,11(4):287-290.
Bode B, Stenlöf K, Harris S, et al. Long-term efficacy and safety of canagliflozin over 104 weeks in patients aged 55-80 years with type 2 diabetes[J]. Diabetes Obes Metab, 2015, 17(3):294-303.
Leiter LA, Cefalu WT, Bruin TW, et al. Dapagliflozin added to usual care in individuals with type 2 diabetes mellitus with preexisting cardiovascular disease: a 24-week, multicenter, randomized, double-blind, placebo-controlled study with a 28-week extension[J]. J Am Geriatr Soc, 2014, 62(7):1252-1262.
Matthaei S, Bowering K, Rohwedder K, et al. Durability and tolerability of dapagliflozin over 52 weeks as add-on to metformin and sulphonylurea in type 2 diabetes[J]. Diabetes Obes Metab, 2015, 17(11):1075-1084.
Neal B, Perkovic V, de Zeeuw D, et al. Efficacy and safety of canagliflozin, an inhibitor of sodium-glucose cotransporter 2, when used in conjunction with insulin therapy in patients with type 2 diabetes[J]. Diabetes Care, 2015, 38(3):403-411.
Matthaei S, Bowering K, Rohwedder K, et al. Dapagliflozin improves glycemic control and reduces body weight as add-on therapy to metformin plus sulfonylurea: a 24-week randomized, double-blind clinical trial[J]. Diabetes Care, 2015, 38(3):365-372.
Fulcher G, Matthews DR, Perkovic V, et al. Efficacy and Safety of Canagliflozin Used in Conjunction with Sulfonylurea in Patients with Type 2 Diabetes Mellitus: A Randomized, Controlled Trial[J]. Diabetes Ther, 2015, 6(3):289-302.
Merovci A, Solis-Herrera C, Daniele G, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production[J]. J Clin Invest, 2014, 124(2):509-514.
Lee CG, Boyko EJ, Barrett-Connor E, et al. Insulin sensitizers may attenuate lean mass loss in older men with diabetes[J]. Diabetes Care, 2011, 34(11):2381-2386.
Bolinder J, Ljunggren Ö, Johansson L, et al. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin[J]. Diabetes Obes Metab, 2014, 16(2):159-169.
Ross S, Thamer C, Cescutti J, Meinicke T, Woerle HJ, Broedl UC. Efficacy and safety of empagliflozin twice daily versus once daily in patients with type 2 diabetes inadequately controlled on metformin: a 16-week, randomized, placebo-controlled trial[J]. Diabetes Obes Metab, 2015,17(7):699-702.
Roden M, Merker L, Christiansen AV, et al. Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naïve patients with type 2 diabetes: a double-blind extension of a Phase III randomized controlled trial[J]. Cardiovasc Diabetol, 2015, 14:154.
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes[J]. N Engl J Med, 2015, 373(22):2117-2128.
Bode B, Stenlöf K, Sullivan D, et al. Efficacy and safety of canagliflozin treatment in older subjects with type 2 diabetes mellitus: a randomized trial[J]. Hosp Pract (1995), 2013, 41(2):72-84.
Chilton R, Tikkanen I, Cannon CP, et al. Effects of empagliflozin on blood pressure and markers of arterial stiffness and vascular resistance in patients with type 2 diabetes[J]. Diabetes Obes Metab, 2015, 17(12):1180-1193.
田丽,王琼英,孙润民, 等.SGLT2i对2型糖尿病合并高血压患者24 h动态血压影响的荟萃分析[J].中华心血管病杂志,2021,49(10):1000-1011.
Oelze M, Kröller-Schön S, Welschof P, et al. The sodium-glucose co-transporter 2 inhibitor empagliflozin improves diabetes-induced vascular dysfunction in the streptozotocin diabetes rat model by interfering with oxidative stress and glucotoxicity[J]. PLoS One, 2014, 9(11):e112394.
Ahmadieh H, Azar S. Effects of Sodium Glucose Cotransporter-2 Inhibitors on Serum Uric Acid in Type 2 Diabetes Mellitus[J]. Diabetes Technol Ther, 2017, 19(9):507-512.
Zhao Y, Xu L, Tian D, et al. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: A meta-analysis of randomized controlled trials[J]. Diabetes Obes Metab, 2018, 20(2):458-462.
Hao Z, Huang X, Shao H, et al. Effects of dapagliflozin on serum uric acid levels in hospitalized type 2 diabetic patients with inadequate glycemic control: a randomized controlled trial[J]. Ther Clin Risk Manag, 2018, 14:2407-2413.
Kanji T, Gandhi M, Clase CM, et al. Urate lowering therapy to improve renal outcomes in patients with chronic kidney disease: systematic review and meta-analysis[J]. BMC Nephrol, 2015, 16:58.
Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes[J]. N Engl J Med, 2017, 377(7):644-657.
Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes[J]. N Engl J Med, 2019, 380(4):347-357.
Cannon CP, Pratley R, Dagogo-Jack S, et al. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes[J]. N Engl J Med, 2020, 383(15):1425-1435.
Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study[J]. Am J Cardiol, 1974, 34(1):29-34.
Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy[J]. N Engl J Med, 2019, 380(24):2295-2306.
Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease[J]. N Engl J Med, 2020, 383(15):1436-1446.
Barnett AH, Mithal A, Manassie J, et al. Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease: a randomised, double-blind, placebo-controlled trial[J]. Lancet Diabetes Endocrinol, 2014, 2(5):369-384.
Tikkanen I, Narko K, Zeller C, et al. Empagliflozin reduces blood pressure in patients with type 2 diabetes and hypertension[J]. Diabetes Care, 2015, 38(3):420-428.
Rosenstock J, Ferrannini E. Euglycemic Diabetic Ketoacidosis: A Predictable, Detectable, and Preventable Safety Concern With SGLT2 Inhibitors[J]. Diabetes Care, 2015, 38(9):1638-1642.
Handelsman Y, Henry RR, Bloomgarden ZT, et al. American association of clinical endocrinologists and american college of endocrinology position statement on the association of SGLT-2 inhibitors and diabetic ketoacidosis[J]. Endocr Pract, 2016, 22(6):753-762.
Yabe D,Nishikino R,Kaneko M,et,al.Short-term impacts of sodium/glucose co-transporter2 inhibitors in Japanese clinical practice:considerations for their appropriate use to avoid serious adverse events[J].Expert Opin Drug Saf, 2015,14(6):795-800.
Sugiyama S, Jinnouchi H, Kurinami N, et al.Dapagliflozin Reduces Fat Mass without Affecting Muscle Mass in Type 2 Diabetes[J].J Atheroscler Thromb, 2018, 25(6):467-476.
Ruanpeng D, Ungprasert P, Sangtian J, et al. Sodium-glucose cotransporter 2 (SGLT2) inhibitors and fracture risk in patients with type 2 diabetes mellitus: A meta-analysis[J]. Diabetes Metab Res Rev, 2017, 33(6). 无页码
Tang HL, Li DD, Zhang JJ, et al. Lack of evidence for a harmful effect of sodium-glucose co-transporter 2 (SGLT2) inhibitors on fracture risk among type 2 diabetes patients: a network and cumulative meta-analysis of randomized controlled trials[J]. Diabetes Obes Metab, 2016, 18(12):1199-1206.
Schwartz AV, Johnson KC, Kahn SE, et al. Effect of 1 year of an intentional weight loss intervention on bone mineral density in type 2 diabetes: results from the Look AHEAD randomized trial[J]. J Bone Miner Res, 2012, 27(3):619-627.
Ruscica M, Baldessin L, Boccia D, et al. Non-insulin anti-diabetic drugs: An update on pharmacological interactions[J]. Pharmacol Res, 2017, 115:14-24.
Devineni D, Polidori D. Clinical Pharmacokinetic, Pharmacodynamic, and Drug-Drug Interaction Profile of Canagliflozin, a Sodium-Glucose Co-transporter 2 Inhibitor[J]. Clin Pharmacokinet, 2015, 54(10):1027-1041.
May M, Schindler C. Clinically and pharmacologically relevant interactions of antidiabetic drugs[J]. Ther Adv Endocrinol Metab, 2016, 7(2):69-83.
Gu N, Park SI, Chung H, et al. Possibility of pharmacokinetic drug interaction between a DPP-4 inhibitor and a SGLT2 inhibitor[J]. Transl Clin Pharmacol, 2020, 28(1):17-33.
Fediuk DJ, Nucci G, Dawra VK, et al. Overview of the Clinical Pharmacology of Ertugliflozin, a Novel Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitor[J]. Clin Pharmacokinet, 2020,59(8):949-965.
Zaccardi F, Webb DR, Htike ZZ, Youssef D, Khunti K, Davies MJ. Efficacy and safety of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes mellitus: systematic review and network meta-analysis[J]. Diabetes Obes Metab, 2016,18(8):783-794.
Devineni D, Vaccaro N, Murphy J, et al. Effects of rifampin, cyclosporine A, and probenecid on the pharmacokinetic profile of canagliflozin, a sodium glucose co-transporter 2 inhibitor, in healthy participants[J]. Int J Clin Pharmacol Ther, 2015,53(2):115-128.
Devineni D, Manitpisitkul P, Murphy J, et al. Effect of food on the pharmacokinetics of canagliflozin, a sodium glucose co-transporter 2 inhibitor, and assessment of dose proportionality in healthy participants[J]. Clin Pharmacol Drug Dev, 2015, 4(4):279-286.
Kasichayanula S,Liu X,Zhang W,et al. Effect of a high-fat meal on the pharmacokinetics of dapagliflozin,a selective SGLT2 inhibitor,in healthy subjects[J]. Diabetes Obes Metab, 2011, 13 ( 8 ) :770-773.
Macha S, Jungnik A, Hohl K, Hobson D, Salsali A, Woerle HJ. Effect of food on the pharmacokinetics of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, and assessment of dose proportionality in healthy volunteers[J]. Int J Clin Pharmacol Ther, 2013, 51(11):873-879.
Sahasrabudhe V, Fediuk DJ, Matschke K, et al. Effect of Food on the Pharmacokinetics of Ertugliflozin and Its Fixed-Dose Combinations Ertugliflozin/Sitagliptin and Ertugliflozin/Metformin[J]. Clin Pharmacol Drug Dev, 2019,8(5):619-627.
